




Peptide therapies have become one of the most discussed topics in longevity, recovery, body composition, and performance medicine. While CJC-1295, Ipamorelin, Sermorelin, and IGF-1 LR3 are often grouped together, they actually work at different points along the body's natural Growth Hormone (GH) and Insulin-Like Growth Factor-1 (IGF-1) pathway.
Understanding where each peptide acts can help explain why some compounds are used together, why their effects differ, and why they are not interchangeable.
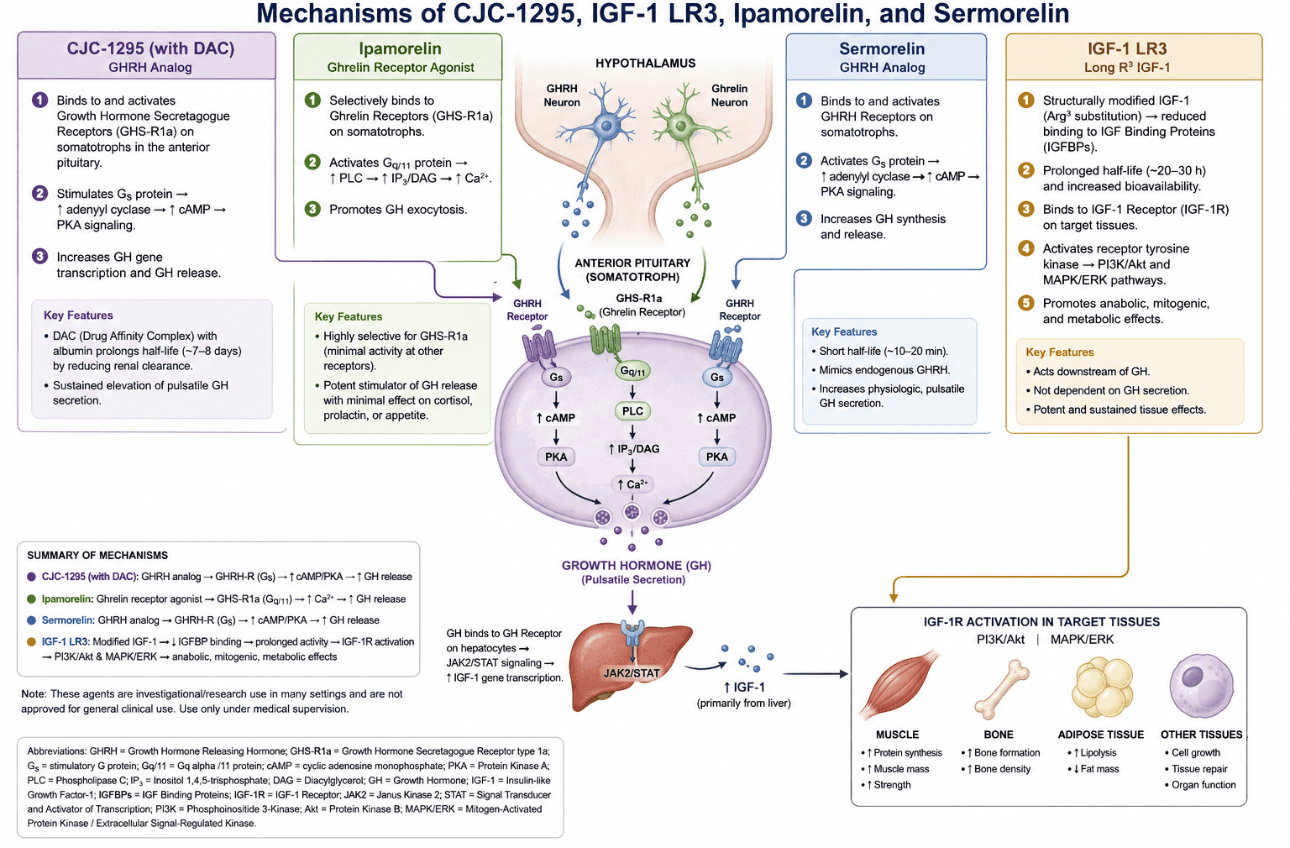
The Growth Hormone–IGF-1 Axis Explained
The body regulates growth hormone through a highly coordinated signaling network.
The process begins in the hypothalamus, a region of the brain that releases signaling molecules that communicate with the pituitary gland. The pituitary then releases Growth Hormone (GH) into circulation. Growth Hormone travels to the liver and other tissues where it stimulates production of Insulin-Like Growth Factor-1 (IGF-1).
IGF-1 is responsible for many of the downstream effects associated with growth hormone, including:
- Muscle protein synthesis
- Recovery from exercise
- Bone remodeling
- Tissue repair
- Fat metabolism
- Cellular growth signaling
Each peptide discussed below influences this pathway differently.
How Sermorelin Works
Sermorelin is a synthetic version of Growth Hormone Releasing Hormone (GHRH).
It acts at the pituitary gland by binding to GHRH receptors located on somatotroph cells. Once activated, these receptors increase cyclic AMP (cAMP) signaling inside the cell, leading to the synthesis and release of Growth Hormone.
Key characteristics of Sermorelin:
- Mimics the body's natural GHRH signal
- Stimulates physiologic GH pulses
- Short half-life
- Depends on a functioning pituitary gland
- Promotes endogenous GH production rather than replacing it
Because Sermorelin works upstream in the GH pathway, it relies on the body's existing hormone-producing machinery.
How CJC-1295 Works
CJC-1295 is also a GHRH analog, but it has been modified to remain active significantly longer than Sermorelin.
The most common version, CJC-1295 with DAC (Drug Affinity Complex), binds to albumin in the bloodstream and remains active for several days.
Like Sermorelin, CJC-1295 stimulates GHRH receptors on pituitary somatotrophs. This leads to:
- Increased cAMP signaling
- Enhanced GH synthesis
- Increased pulsatile GH secretion
- Elevated downstream IGF-1 production
Key characteristics of CJC-1295:
- Longer half-life than Sermorelin
- Sustained GH stimulation
- Increased endogenous IGF-1 production
- Often paired with growth hormone secretagogues such as Ipamorelin
Many clinicians view CJC-1295 as an extended-duration version of the body's natural GHRH signal.
How Ipamorelin Works
Ipamorelin works through a completely different receptor.
Instead of targeting GHRH receptors, it binds to Growth Hormone Secretagogue Receptors (GHS-R1a), commonly known as ghrelin receptors.
Activation of these receptors triggers:
- Phospholipase C signaling
- Increased intracellular calcium
- Growth hormone release from pituitary somatotrophs
Why Ipamorelin is different: Ipamorelin is considered one of the most selective GH secretagogues currently available. Unlike older compounds in the same class, it has relatively little activity on:
- Cortisol secretion
- Prolactin secretion
- Appetite stimulation
This selectivity is one reason it remains popular in peptide protocols.
Why CJC-1295 and Ipamorelin Are Often Combined
The two peptides activate separate signaling pathways that converge on Growth Hormone release.
- CJC-1295 activates the GHRH receptor pathway
- Ipamorelin activates the ghrelin receptor pathway
Because both pathways stimulate pituitary somatotrophs through different mechanisms, they may work synergistically to increase physiologic GH pulses.
A simplified model:
GHRH Pathway (CJC-1295) ─┐
├──→ Enhanced GH Pulsatility
Ghrelin Pathway (Ipamorelin) ─┘
This complementary mechanism explains why the combination is frequently discussed in performance and longevity communities.
How IGF-1 LR3 Works
IGF-1 LR3 is fundamentally different from the other compounds on this list.
Instead of stimulating Growth Hormone release, IGF-1 LR3 acts downstream of GH. It is a modified version of insulin-like growth factor-1 engineered to:
- Resist binding proteins
- Remain active longer in circulation
- Increase tissue exposure
Once administered, IGF-1 LR3 binds directly to IGF-1 receptors in tissues throughout the body. This activates intracellular pathways including:
PI3K/Akt Pathway — associated with muscle protein synthesis, cellular growth, and metabolic regulation.
MAPK/ERK Pathway — associated with cell proliferation, tissue repair, and growth signaling.
Because IGF-1 LR3 acts downstream, it bypasses the pituitary growth hormone release process entirely.
Comparing These Four Peptides
| Compound | Primary Target | Main Effect | |---|---|---| | Sermorelin | GHRH Receptor | Stimulates endogenous GH release | | CJC-1295 | GHRH Receptor | Sustained GH stimulation | | Ipamorelin | Ghrelin Receptor (GHS-R1a) | Triggers GH secretion | | IGF-1 LR3 | IGF-1 Receptor | Direct tissue-level IGF signaling |
For a deeper dive into the specific compounds available, see our Peptide Therapy Education page, which catalogs 23 active peptide compounds with full mechanism-of-action references.
Frequently Asked Questions
Is IGF-1 LR3 the same as Growth Hormone?
No. Growth Hormone stimulates the body to produce IGF-1. IGF-1 LR3 acts downstream and directly activates IGF-1 receptors.
What is the difference between Sermorelin and CJC-1295?
Both stimulate the GHRH receptor, but CJC-1295 is engineered to remain active significantly longer.
Why do people combine CJC-1295 and Ipamorelin?
They target different receptors involved in Growth Hormone release, creating complementary signaling pathways.
Does IGF-1 LR3 require Growth Hormone release?
No. IGF-1 LR3 acts independently of pituitary GH secretion.
Which peptide works directly on muscle tissue?
IGF-1 LR3 is the compound that most directly targets IGF-1 receptors within muscle and other peripheral tissues.
The Bottom Line
Although CJC-1295, Sermorelin, Ipamorelin, and IGF-1 LR3 are frequently discussed together, they operate at different levels of the Growth Hormone–IGF-1 axis.
- Sermorelin and CJC-1295 mimic the body's natural GHRH signal
- Ipamorelin mimics ghrelin receptor activation to promote GH release
- IGF-1 LR3 bypasses Growth Hormone production altogether and acts directly on IGF-1 receptors in target tissues
Understanding these mechanisms helps explain why each compound produces different physiologic effects and why they are often used in different clinical and research settings.
If you're researching peptides as part of a broader recovery or longevity plan, you may also find these resources useful:
- BPC-157 vs GHK-Cu vs TB-500 — mechanisms behind tissue repair peptides
- Epitalon vs Kisspeptin-10 vs NAD+ — longevity pathways explained
- AOD-9604 vs MOTS-c vs Tesamorelin vs Semaglutide vs Tirzepatide — weight loss & metabolic peptides
- DSIP Peptide for Sleep — delta sleep, HPA-axis, and recovery
- KPV vs LL-37 vs Thymosin Alpha-1 — immune-supporting peptides
- Peptide Therapy Education — 23 active compounds
- Stem Cell Therapy for Degenerative Disc Disease
- Advanced Neuromodulation for Chronic Pain on Long Island
Curious Whether Peptide Therapy Fits Your Goals?
Peptides are not interchangeable, and the right protocol depends on your physiology, medical history, and what you're actually trying to optimize — energy, recovery, body composition, longevity, or something more specific. A single consultation can cut through the noise.
Dr. Rubin sees patients at our Garden City and New Hyde Park offices and serves the greater Nassau County and Queens area. Call 516-492-3100 or text 516-206-0774 to schedule a consultation, or complete the peptide intake form online before your visit to save time in the office.
Medical Disclaimer
The information provided in this article is for educational purposes only and should not be interpreted as medical advice. Peptide therapies may not be appropriate for every patient. These agents are investigational or research use in many settings and are not approved for general clinical use. Always consult a qualified healthcare professional before beginning any treatment program.
Written by Dr. Edward Rubin, MD — board-certified in Pain Medicine and Anesthesiology, with fellowship training at Cornell, Columbia, Hospital for Special Surgery, and Memorial Sloan Kettering. Dr. Rubin has been treating patients on Long Island for over 20 years.